Because @jfoy.bsky.social asked for it, it is time for Linear-No Threshold (LNT) Hypothesis & As Low As Reasonably Acheivable (ALARA) chat. One is a philosophy and the other is a model operating within that philosophy.
NOTE: If you have a burning and irresistable desire to chime in about the beneficial effects of radiation hormesis just…don’t. Go talk to Dan Kaszeta about nerve agents instead.
The underpinning philosophy of ionizing radiation work is that we will keep doses As Low As Reasonably Achievable (ALARA). When we first developed the tools to monitor radiation, the philosophy was to keep dose As Low As Possible (ALAP) with a side order of no real dose limits. Working to ALAP means you will spend tremendous amounts of money preventing radiation exposure that appeared to have no deleterious effects for no gain, i.e. it was already wasn’t hurting anything, but you spent millions to make it [reads notes] still not hurt anything but the number is lower? Cool.
But the ALAP philosophy demands that if you can make that number lower, you must. This was felt to be overly restrictive and far too expensive/time consuming by the nascent nuclear industry and Atomic Energy Commission which was trying to promote it’s development. This is how it changed into ALARA.
The problem with ALARA is that the words “Reasonably” and “Acheivable” are very subjective concepts. Many legal, regulatory, and scientific careers have been built arguing them since the Atomic Energy Act of 1954 was signed and dose limits coming into existence. Reasonable is mostly definited in a financial sense. What is a bankrupting expense for very little reduction in dose for a small company may be normal business operations for a national laboratory. This gets derisively called “The Million Dollar Millirem” in DOEland, chasing what seems like inconsequential dose. Except that dose is a clue.
When you see dose you don’t expect, even if it seems inconsequential, you have to stop and question is the dosimetry working right. Is this just noise? If it looks good, you start asking about work practices. Did Bob do something out of the ordinary? Did Bob not follow the procedures? Then you move to the systemic causes. Is there a source where it shouldn’t be? Has shielding been altered? Is a control system or such, somewhere failing? Sleuthing like that gets expensive in hours quick but the consequence of missing an indicator at a nuclear facility is more severe than other places. But do you HAVE the staff to even do that sleuthing? The equipment? The time and money? Or do you shrug and say “Eh, we’re under the dose limits. We’re fine.” This is why careers are built on arguing about Reasonable and Achievable.
Philosophically, under ALARA, you should at least try to make an effort to keep doses low not just give up at the slightest difficulty and roast your people right up to the occupation dose limit (50mSv in the US). This is asking a lot of the management mindset, I know. But as anyone who has dealt with That Guy before IN ABSOLUTELY ANY SCENARIO before knows, any limit is a challenge to their freedom. They will work to that limit out of spite. They will test that limit to see if there’s any give. They will evade any metrics that might show they’ve done wrong.
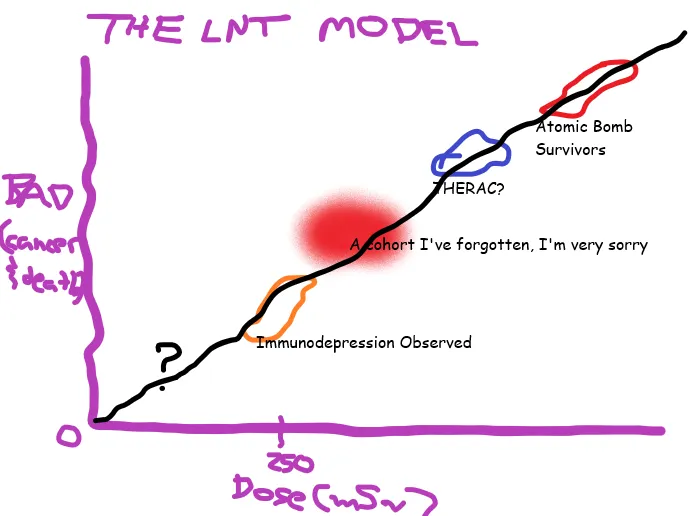
In general, people are not mad with ALARA as a dose mitigation philosophy. What they are mad at are limits, any limits, and the framework of the Linear-No Threshold (LNT) Hypothesis that underpins it because there are some inconvenient things pop out when you combine ALARA, LNT, and a limit together. LNT is an a dose/health effects(read: injury or death) model were you make a simple graph plotting ionizing radiation dose versus likelihood/severity of the effect. And then you draw a line through all the victim cohorts down through the origin, hence Linear.
Now, as anyone that has had to play with statistics and drawing graphs knows, the error bars on data points mean your best fit line to go through them all is up to some interpretation. If you have something that really doesn’t fit, can you ignore that point as an outlier? What if you have a region where there are no data points? Is it okay to extend your plot through this region? This is one of the argument points against the LNT: not a lot of data points as you get close to the origin. For the radiation health effects graph, we have a excellent and definitive date at high, acute doses. We have cohorts of victims that demonstrate a nice, linear “Increased Dose = Increased Injury” response. It gets very messy in the lower dose ranges or you instead want to talk about chonic doses.
Since the very earliest days of trying to set a dose limit, there were arguments about what that limit should be. Is there a dose below which there is no effect, a Threshold? It’d mean we don’t have to chase dose if they don’t matter. “Look, we can’t even see any biological effects below 250mSv.” And that statement, which I’ve heard many times even from fellow health physicists, was accurate…in the 1960s. One of my favorite sayings is “There is a world of difference between detectable & dangerous and our detectors get better every year.” We’ve also gotten better at finding effects.
Are the lower dose biological effects we can now detect consequential? Maybe, maybe not. But the point is we CAN notice them which means we’re shining a flashlight on the former No Data Here part of the graph which makes drawing that line from Hiroshima & Nagasaki victims down to the origin look better. Where people would have once liked to set a threshold is now a place we have data below, which would have invalidated that threshold, building the argument that there is No Threshold. The next argument point is what if you draw curves rather than lines? Sure, you can try to fit anything you like to the datapoints you’ve got and that does carry some freight as to health consequence and controls you’d want to do to try to keep doses ALARA. Except the people arguing against LNT want to do less work, have less controls. Guess how those curves look.
The dose limit we currently work under in the United States is not the same as the rest of the world nor has it always been the limit that it is today. Over the decades, those limits have dropped to 50mSv for radiation workers and .1mSv for the general public. The 50mSv rad worker limit was chosen to be 1/5 of the lowest observed acute radiation exposure biologial effect when it was initially recommended in the 1950s, though not formally adopted until the 1970s. If you’ve driven that lowest observable threshold down, shouldn’t the limit ratchet down too? A lowered limit is very much not the desire from people that want LNT to go away. They want the limit and the arguments underpining it to go away. Yes, the limit and LNT hypothesis is conservative but that’s kinda what you want in safety models. Arguing against LNT is what they chose to attack.
Consider this an analgous tactic to arguing definitions of when life begins for abortion debates to attack legislaton and case law you don’t like. Indirect methods. ~fin~
Well, no. For pure Phil opinion, if you’re not actively doing the research to change it, a health physicist arguing to get rid of the LNT is trying to avoid work. The techbros arguing for it have a TESCREAL bent where everyone but them is expendable. And a poor command of the history of the field.